


What is Crohn’s Disease?
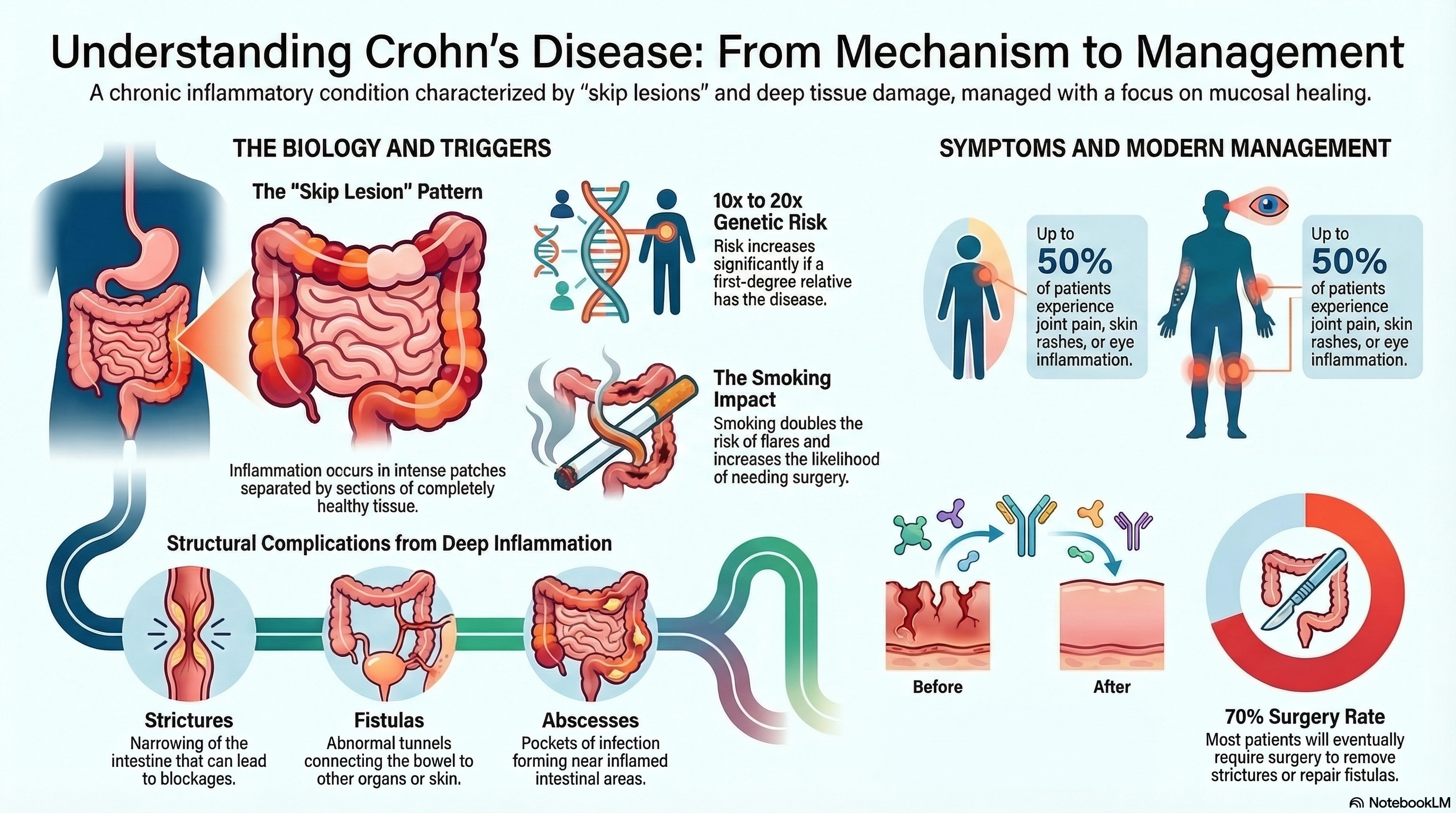
Crohn’s disease is characterized by "skip lesions," which means you may have patches of intense inflammation followed by sections of completely healthy tissue. It most frequently involves the terminal ileum (the end of the small intestine) and the proximal colon (the beginning of the large intestine).
Because the inflammation is so deep, the body’s attempt to heal can lead to significant structural changes, such as:
-
Strictures: Narrowing of the intestine that can lead to blockages.
-
Fistulas: Abnormal tunnels or connections between the bowel and other organs, such as the bladder, skin, or other parts of the intestine.
-
Abscesses: Pockets of infection that form near the inflamed areas.
Causes of Crohn’s Disease
The exact cause is unknown, but it is widely understood to be an "inappropriate" immune response where the body attacks its own intestinal microbes.
-
Genetics: There is a strong hereditary link. If you have a first-degree relative with Crohn’s, your risk is 10 to 20 times higher. Researchers have identified over 260 genetic markers, including the NOD2 mutation, that contribute to the disease.
-
Racial and Ethnic Factors: The disease is most prevalent in Caucasians and individuals of Ashkenazi Jewish descent. However, incidence rates are rising globally across all ethnic groups.
-
The Microbiome: Patients typically have "dysbiosis," or a lack of diversity in their gut bacteria, specifically a reduction in helpful, anti-inflammatory bacteria.
-
Environmental Triggers: Smoking is the most significant modifiable risk factor. It doubles the risk of flares and increases the likelihood that a patient will need surgery.
Symptoms of Crohn’s Disease
Symptoms can range from mild to severe and often go through periods of "flare-ups" and remission.
-
Chronic Diarrhea: This is often the most persistent symptom and can occur at night.
-
Abdominal Pain: Usually felt in the lower right side of the abdomen.
-
Weight Loss and Fatigue: Caused by both a loss of appetite and the body’s inability to absorb nutrients properly.
-
Perianal Disease: Approximately 30% to 50% of patients develop painful sores, fissures, or drainage (fistulas) around the anal area.
-
In Children: Growth failure and delayed puberty may be the very first signs of the disease.
Extraintestinal Manifestations: Because Crohn’s is an immune-mediated disease, it can affect parts of the body outside the gut. Up to 50% of patients experience joint pain (arthritis), skin rashes (erythema nodosum), or eye inflammation (uveitis).
Diagnosis of Crohn’s Disease
There is no single "gold standard" test for Crohn’s. Doctors use a "jigsaw puzzle" approach, combining several pieces of evidence to confirm the diagnosis.
-
Endoscopy and Colonoscopy: This allows doctors to see the classic "cobblestone" appearance of the intestinal lining and take biopsies (small tissue samples).
-
Imaging: MR Enterography or CT scans are used to look at the small intestine and check for deep inflammation or fistulas that a scope cannot reach.
-
Stool Tests: A test for fecal calprotectin is the best non-invasive way to measure active inflammation in the gut.
-
Blood Tests: These check for anemia (low iron), high inflammatory markers (CRP), and vitamin deficiencies (B12 and D).
Treatment of Crohn’s Disease
The goal of modern treatment is not just to "feel better," but to achieve mucosal healing—repairing the lining of the gut to prevent long-term damage.
-
Biologics: These are the current cornerstone of therapy. They target specific proteins in the immune system to stop inflammation. Common classes include anti-TNF agents (Infliximab, Adalimumab) and newer IL-23 inhibitors like Risankizumab (Skyrizi).
-
Small Molecules: Newer oral medications like Upadacitinib (Rinvoq) are highly effective for moderate-to-severe cases.
-
Corticosteroids: Drugs like Prednisone are used to quickly "put out the fire" during a flare but are not used for long-term maintenance due to side effects.
-
Surgery: Approximately 70% of patients will require surgery at some point in their lives, often to remove a stricture or repair a fistula. While surgery can provide years of relief, it is not a "cure," as the disease can return.
Prevention of Crohn’s Disease
While you cannot prevent the genetic onset of Crohn’s disease, you can take significant steps to manage its severity and prevent complications.
-
Smoking Cessation: This is the most important lifestyle change. Quitting smoking significantly reduces the severity of the disease and the need for repeated surgeries.
-
Early Intervention: Seeking treatment as soon as symptoms appear ("Treat-to-Target") is the best way to prevent the permanent scarring and fistulas that lead to surgery.
-
Nutritional Support: While no specific diet cures Crohn’s, working with a dietitian to identify "trigger foods" and ensuring you get enough Vitamin D and B12 can prevent malnutrition.
-
Cancer Surveillance: If your colon is affected, you should have a screening colonoscopy every 1 to 2 years once you have had the disease for 8 to 10 years, as there is an increased risk of colorectal cancer.


